Continuing Education At Home
Professional Counselor - MFT - NBCC
Parkinson's Disease
See Accreditations - click here
There is no known conflict of interest or commercial support related to this CE program.
Course Description
This course is destined to all health-care professionals wishing to gain additional knowledge on Parkinson's Disease and improve their practice. Parkinson's Disease (PD) is a degenerative condition of the brain associated with motor symptoms (slow movement, tremor, rigidity and imbalance) and other complications including cognitive impairment, mental health disorders, sleep disorders and pain and sensory disturbances. It also affects dopamine receptors and is therefore associated with an increased risk of depression. Globally, disability and death due to Parkinson's Disease are increasing faster than for any other neurological disorder. The prevalence of PD has doubled in the past 25 years, and global estimates in 2019 showed over 8.5 million individuals with PD (WHO, 2019).
This training covers early manifestations of the disease, medical treatment options, rehabilitation, work and life adjustments as well as the stages of grief and reactions to the diagnosis, thus providing the reader with a solid understanding of PD and the medical approaches that can be undertaken.
Introduction
Parkinson’s disease is neurodegenerative disorder that causes difficulties with movement and behavior that become progressively worse over time. It is one of the most common neurological disorders affecting about 1 percent of people over the age of 60 and is the second most common movement disorder. Parkinson’s disease manifests itself in several characteristics ways including a resting tremor, cogwheel rigidity and postural instability. Other common features are “masked facies,” a poverty of movement and the phenomenon of “freezing.” Many of the neurological problems associated with Parkinson’s disease can be linking to a destruction of dopamine-containing neurons in a region of the brain called the substantia nigra. Perhaps the current most famous person with the disease is the actor Michael J. Fox, who has raised public awareness about the disease and continues to work toward raising money for research.
Origins
James Parkinson first described the disease that bears his name in 1817. He published under the title “An Essay on the Shaking Palsy” and used that venue to describe six cases of the disease. He describes the disease as “involuntary tremulous motion, with lessened muscular power, in parts not in action and even when supported; with a propensity to bend the trunk forwards, and to pass from a walking to a running pace: the senses and intellects being uninjured.” Many of the symptoms that he described are used in diagnosis today. Importantly, he differentiated this disorder from other illnesses that resulted in “shaking palsy” such as epilepsy. His work was one of the earliest descriptions of any neurological disorder and heralded an era classification and description that accelerated the practice of modern neurology.
Parkinson’s disease is occasionally referred to a paralysis agitans as it was known in Dr. Parkinson’s the time, though its use now is mostly a historical reference.
Incidence and Prevalence
The incidence of Parkinson’s disease is estimated to be between 5 and 20 cases per 100,000 people each year. The overall prevalence in the United States is about 120-150 patients per 100,000 people. The disease is slightly more prevalent in men than in women occurring about 1.5 times as often in the former gender. The average age at onset is 60 years and the disease is rarely seen in patients under the age of 40. Instances of Parkinson’s disease symptoms produced by exogenous or environmental toxins are the obvious exceptions.
Symptoms
Early Manifestations
Researchers have attempted to identify certain symptoms that predate the onset of classic movement symptoms. Unfortunately, many of these are non-specific and therefore not terribly helpful. For example, clinicians have noticed that people that are destined the develop Parkinson’s disease are excessively sleepy during the daytime and have recurrent issues with constipation. Depression may also occur before movement symptoms are present. These symptoms are, of course, nonspecific. Other symptoms that precede overt Parkinson’s disease symptoms may prove to be useful screening tools. Patients with Parkinson’s disease display problems in their sense of smell long before tremors occur. Also, disturbances in REM sleep are quite common in Parkinson’s disease and often begin years before classic Parkinson’s disease symptoms. REM behavior disorder is a disorder in which the normal atonia, or loss of muscle tone that occurs during REM sleep is lost. In one study nearly four out of ten men in their fifties that displayed REM behavior disorder went on to develop Parkinson’s disease. Currently there is no accurate means to diagnose Parkinson’s disease prior to the onset of the cardinal symptoms. As more information is learned about the genetics of the disease, a test may be developed that can make the diagnosis of Parkinson’s disease earlier.
Cardinal Features
There are essentially three cardinal features of Parkinson’s disease that are present early in the disease, two of which need to be present in order to make the diagnosis. The disease is characterized by a resting tremor, rigidity and bradykinesia. Later in the course of the disease, usually almost a decade after symptom onset, another cardinal feature of the disease emerges which is postural instability.
The resting tremor almost always begins asymmetrically i.e. on one side of the body. A tremor that begins symmetrically calls the diagnosis of Parkinson’s disease into question and may be more consistent with essential tremor or other disorder. The resting tremor is classically described as a “pill-rolling tremor” since it seems as if the patient is rolling a pill between the thumb and first finger. The tremor is predictably between 3 to 5 Hz such that the oscillations of the hand can be counted off about four times per second. About a fifth of patients with Parkinson’s disease first notice clumsiness in the affected hand prior to the onset of a noticeable tremor.
The tremor in Parkinson’s disease is a resting tremor and is most severe when the patient’s limb is at rest. A distinction is made between a resting tremor and a postural tremor or action tremor. The tremor of Parkinson’s disease actually improves with directed action. In other words, the tremor can be minimized when the patient is asked to perform a specific task requiring manual dexterity, yet returns after the task is completed. This is not to say that the tremor does not interfere with activity—it certainly does—coordination in the affected hand and arm is usually compromised. Also, since the tremor is present at rest, it may also be present during tests of postural tremor and can complicate the differential diagnosis. Strong clues that the disorder is actually Parkinson’s disease are that the tremor is asymmetric at presentation and occurs when the limb is completely at rest.
As we will discuss, the resting tremor is usually very responsive to treatment with dopaminergic agents and their benefit can help to reinforce a diagnosis that may be unclear.
Rigidity is another hallmark of the disease and has traditionally been described as cogwheel rigidity. This eponym is used to describe the sensation that one feels as they attempt to straighten an affected patient’s arm. Patients with Parkinson’s disease will be asked to hold their arms bent at a 90 degree angle but not to provide active resistance to the examiner’s movement. As the physician attempts to straighten the patient’s arm, there is a lead pipe resistance to movement that is not being activated by the patient deliberately. The cogwheeling (i.e. the stuttering resistance with relaxation) is thought to be caused by the patient’s tremor acting across the elbow. The rigidity is certainly present in Parkinson’s disease but not in the same way or to the same degree as it is in patients with stroke in which the arm is constantly contracted and cannot be overcome by the examiner unless significant force is applied (clasp knife rigidity). Given the subtlety of this rigidity in some patients, the patient may be asked to perform a moderately complex task with the contralateral arm in order to accentuate the rigidity in the ipsilateral arm. For example, if the tester wants to examine rigidity in the patient’s right arm, she will ask the patient to draw circles in the air with the index finger of the left hand. While the patient attends to the task with the left arm, the patient’s right arm is being moved by the tester.
Bradykinesia essentially means decreased movement and is another hallmark of Parkinson’s disease. Patients will often take a significant amount of time to complete tasks and will not engage in spontaneous movements as most would. Bradykinesia may be mistaken for depression, apathy or even laziness but is truly a sign of the movement disorder. In addition to a general poverty of movement, more subtle evidence of bradykinesia usually exists. One tell-tale sign of bradykinesia in Parkinson’s disease is the presence of a phenomenon called micrographia. Doctors ask the patient with presumed Parkinson’s disease to write a sentence of their own creation. After a pause (another feature of the disease), the patient often writes individual letters much smaller than most people would and also much smaller than the patient used to write prior to the start of the disease. Obviously, previous writing samples may be required in order to verify this bradykinetic change. Other subtle bradykinesias include a decreased blink rate and soft speech (hypophonia).
Another of the more noticeable bradykinesias is referred to as “masked facies.” In this manifestation of the disease, patients are unable to smile in the normal course of conversation or the degree to which they smile is severely dampened. This phenomenon of masked facies is particularly troubling to patients and their families because patients lose a large part of their ability to communicate through non-verbals. Smiling is affected but also signs of normal emotions are not present in the face. While patients with Parkinson’s disease continue to experience a full range of emotions for much of the disease course, the ability to facially express these emotions is severely impaired.
Postural instability is a later manifestation of Parkinson’s disease but is almost always present if the patient lives long enough. While it is not considered one of the three diagnostic criteria, the classic finding of postural instability seen in Parkinson’s disease often manifests as a shuffling gait. Patients will walk with a stooped posture and the pads of the feet will skim across the ground. Steps that are taken lack apparent confidence. It is very common for patients with Parkinson’s disease to stoop and lean so far forward while at the same time not placing their feet far enough in front of their mass that they appear to briefly race forward and fall forward as their center of gravity shifts forward and leaves the area supported by their feet. Dr. Parkinson described this behavior in 1817 as passing “from a walking to a running pace.” This change in pace is essentially the body trying to accommodate the shifting body weight.
One test of postural stability is to have the patient turn around in a narrow passageway, such as a hall. Most people will need very few steps to accomplish this feat but patients with moderately advanced Parkinson’s disease require several and appear unsteady as they do so. Also, neurologists will sometimes jar a person backwards to test their ability to equilibrate to a sudden change in posture. Again, normal people will require usually no more than one backward step and many will be able to employ muscles in their trunk to prevent backward motion. Patients with Parkinson’s disease usually require several steps and eventually lose their balance completely and fall into the waiting arms of their physician.
Common Symptoms of Parkinson’s Disease
One of the more bizarre symptoms of Parkinson’s disease is a behavior known as freezing. Later in the course of the disease, patients will be unable to rise from a seated position despite a desire to do so. It is not that they lack the trunk or leg strength to accomplish the task, but rather they are unable to activate the motor sequence required to accomplish the task. In other words, they want to get up, their legs are strong enough to get them up, but their brain will not fire the right sequence of neurons to get them up. They also may lack the ability to begin to walk out of a room even if they are already standing and attempt to do so. Perhaps one of the most curious examples of freezing occurs when patients come to certain areas in space. For instance, patients with Parkinson’s disease may freeze when they come to the threshold of an open door. They may also freeze when they come to a long corridor. One fascinating finding is that if patients are presented with visual cues on the floor (e.g. pieces of tape forming stripes perpendicular to the path of motion) the corridor that once caused them to freeze can now be traversed with ease. The visual cues circumvent whatever neural process that is taking place that prevents them from walking down the corridor.
In Parkinson’s disease, nerve cells die in other locations besides the substantia nigra. Nerves that provide information about smell, control urination, assure movement of material through the digestive tract and maintain blood pressure can be affected by the disease. It is common for people with Parkinson’s disease to partially lose their sense of smell early in the disease. Urinary incontinence and retention also occur which can lead to bladder infection. Further complicating the issue, urinary tract infection is a major cause of delirium in older individuals and is particularly challenging for patients with Parkinson’s disease. While it sometimes goes unmentioned, erectile dysfunction can occur and may be resistant to pharmacological treatment. Later in the disease, orthostatic hypotension becomes more prominent. Orthostatic hypotension is a drop in blood pressure that occurs with a change in body position from resting to standing. Under normal circumstances, when we rise from a seated position our heart and blood vessels compensate by increasing blood pressure to continue blood flow to the brain. In orthostatic hypotension, this reflex is weak or lost, and blood flow to the brain is inadequate. This compounds the problems that Parkinson’s disease patients have will falls. Not only does Parkinson’s disease cause postural instability, but orthostatic hypotension can lead to transient periods of blacking out as blood is not delivered to the brain.
The stooped posture seen in patients with Parkinson’s disease can lead to unexpected consequences. Since the shoulders are hunched over the chest, the amount of space available to the lungs is decreased thus the amount of air that can be inhaled is decreased. This leads to diminished lung capacity, acid-base disturbances in the blood and possibly to respiratory infections (in severe cases). The chances for respiratory infection also increase because there is a significant amount of dysphagia in later stages of Parkinson’s disease. Just as there is a lack of motility in the gut in Parkinson’s disease, so is there a lack of coordination in swallowing. Usually aggressive speech therapy can improve outcomes, at least in early and middle stages, however a discussion about the implementation of a feeding or gastric tube needs to be discussed when the patient can give informed consent.
Medical professionals and caregivers need to be vigilant for psychiatric disturbances in patients with Parkinson’s disease. These occur as a consequence of the disease but also as a side effect of medicines that affect the brain’s dopamine system. Depression is the most common psychiatric illness seen in Parkinson’s disease and is present in as many as half of those diagnosed with the disease. Because of the poverty of movement and “masked facies” it may be difficult to spot symptoms of depression in patients with Parkinson’s disease. It is important to ask probing questions in terms of mood and behavior. Treating depression in Parkinson’s disease patients can be a challenge pharmacologically. Because they are on so many agents that affect monoaminergic neurotransmission, there may be significant drug interactions with many of the traditional antidepressant medications. Special care must be taken when prescribing tricyclic antidepressants and agents that affect monoamine oxidases and even selective serotonin reuptake inhibitors.
The goal of symptomatic treatment of Parkinson’s disease is to restore dopamine neurotransmission. Too much of a good thing can be a bad thing in this case. If a patient with Parkinson’s disease or a caregiver reports a sudden onset of bizarre behavior, hallucinations, delusions, or confusion the Parkinson’s disease medications must be considered, especially if there is no history of psychiatric illness. However, the disease itself may lead to these symptoms and can be extremely difficult to treat. The mainstay of therapy in patients with psychosis is dopamine receptor antagonists or blockers and many of the treatments for Parkinson’s disease are aimed at improving or augmenting dopamine neurotransmission. The treatment of psychosis in Parkinson’s disease is indeed complicated and may require the combined efforts of neurologists and psychiatrists.
Apathy is another psychiatric feature that is quite common in patients with Parkinson’s disease. Again, apathy is difficult to catch because of the bradykinesia and facial changes seen in the disease. Apathy is considered its own psychiatric symptom and should not be confused with depression. In Parkinson’s disease, apathy is likely the result of the neurodegenerative disease process rather than a reaction to a set of unfortunate consequences. It is present in 10 to 40 percent of patients with Parkinson’s disease at some point in the illness. Apathy should be proactively assessed, identified and treated because it can affect treatment outcomes and quality of life. One scale used to determine apathy is the apathy evaluation scale developed by Mel Glenn, M.D. and colleagues and is available in the Resources section.
Dementia goes hand in hand with Parkinson’s disease. If Parkinson’s disease patients are followed and live long enough, some have argued that dementia will occur in 100 percent. An eight year prospective study found that nearly 80 percent of patients with Parkinson’s disease went on to develop dementia. Given this high rate of comorbidity, it is essential to incorporate dementia testing into patient visits. While treatment of dementia that occurs with Parkinson’s disease is quite difficult, identifying that it exists allows certain patient care strategies to be adopted before the dementia progresses. It is also much easier for caregivers, patients and families to deal with all informed consent decisions prior to the onset of dementia. It is also important to teach families and caregivers about dementia as they are being taught about Parkinson’s disease.
Laboratory and Radiology
The diagnosis of Parkinson’s disease is based on history and physical exam. Currently there is no laboratory test that can definitively diagnose Parkinson’s disease. In some cases, especially those in which the presentation is not classic or completely typical, tests should be done to rule out other causes of Parkinsonism or to identify exogenous factors that may have lead to the Parkinson’s disease symptoms.
A considerable amount of research has been and continues to be conducted to discover a reliable laboratory test for Parkinson’s disease. Researchers have attempted to identify biomarkers that could be used to diagnose Parkinson’s disease either as a confirmatory test or in advance of Parkinson’s disease symptoms. One biomarker that is the focus of much scrutiny is alpha-synuclein, a protein that is accumulates in the brains of patients with Parkinson’s disease and other neurodegenerative diseases. While it is possible to measure alpha-synuclein in various fluids and tissues, its specific correlation to the presence and severity of symptoms in Parkinson’s disease has not been established.
Patients with idiopathic Parkinson’s disease (the basic form of Parkinson’s disease) do not display any characteristic changes in the brain MRI and CT, therefore these studies are usually unnecessary. If the diagnosis is uncertain, an MRI may be useful to rule out vascular (multi-infarct), structural and certain toxic/metabolic etiologies.
In cases where the diagnosis of Parkinson’s disease is in doubt, two nuclear radiology studies are available that can provide information about the dopamine system. Positron emission tomography and (PET) and single photon emission computerized tomography (SPECT) use a radiolabeled tracer to identify degeneration in certain areas of the brain. Dopa, the precursor to dopamine, is labeled with 18-fluorine and is taken up by dopaminergic neurons. This marker is identified through PET and SPECT scans. In the putamen opposite the tremor (contralateral side) 18F-dopa uptake is only about two-thirds that of the ipsilateral side. While this helps to strengthen the diagnosis, this same phenomenon may also occur in other diseases that affect the dopamine system such as PSP (progressive supranuclear palsy) or multiple system atrophy. The value of these nuclear radiological tests is to verify that the dopamine system is affected.
Pathophysiology
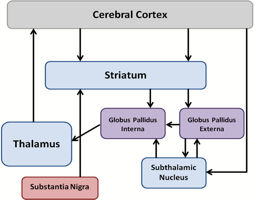
The one feature that is common to every person with Parkinson’s disease is that there is a loss of dopamine-containing neurons in the brain. The area of the brain that is home to most of the dopamine-containing neurons in the brain is the substantia nigra or literally “black substance”. This region of the brain gets its name from the fact that even with the naked eye, this area appears as a black smudge on the normally pale background of brain tissue. The cells of the substantia nigra send axons or projections to many areas of the brain, including the basal ganglia. In the basal ganglia, the primary target for axons coming from the substantia nigra is the striatum (Figure 1). These dopaminergic inputs are important for proper function of the basal ganglia and the basal ganglia, in turn, assures proper motor function. As dopamine containing neurons in the substantia nigra die, the activity of the basal ganglia is affected and the typical difficulties in movement occur. It is not known why these neurons die but it seems that the cause may be linked to both genetics and the environment. Currently there is no way to stop these dopamine-containing neurons from dying and most treatments are simply aimed at correcting movement disorders for as long as possible.
Figure 1 – A Simplified Diagram of the Basal Ganglia and Its Connections.
Arrows indicate projections of axons and neurotransmission can be either excitatory or inhibitory depending on the neurotransmitter system. Proper functioning of this system is important for movement.
The other finding that is seen in patients with Parkinson’s disease is that neurons begin to show intracellular inclusions of abnormal proteins called Lewy bodies. Under that magnification of a microscope they appear to have a dense core and a surrounding halo. Lewy bodies tend to be seen within the substantia nigra of patients with Parkinson’s disease. While Lewy bodies are present in Parkinson’s disease, they also appear in Parkinson-like diseases and other diseases that are clinically similar to Parkinson’s disease. Lewy bodies also form in diseases such as Alzheimer’s disease and can occasionally be seen at autopsy contained within the neurons of elderly people that had no symptoms of Parkinson’s disease or related diseases. Therefore, the presence of Lewy bodies is consistent with Parkinson’s disease but certainly does not rule out other diseases. Lewy bodies are mostly comprised of a protein called alpha-synuclein but also contain other proteins such as ubiquitin. Antibodies against ubiquitin are used to identify Lewy bodies by immunohistochemistry.
The pathways within the basal ganglia are complex and beyond the scope of this training module. However, there are some key facts about the circuits of the basal ganglia that are needed in order to understand the current treatments of the disease. The primary target for dopamine neurons of the substantia nigra is the striatum, one of the major structures of the basal ganglia. Neurons from the substantia nigra release dopamine on neurons of the striatum and control their activity. The striatum, in turn, send axons to other groups of neurons in the basal ganglia including the globus pallidus interna, globus pallidus externa and even back to the substantia nigra. These structures effect movement by sending axons to the thalamus and cerebral cortex. These basal ganglia circuits are a combination of excitatory and inhibitory connections that work in unison to achieve very specific body movements. As neurons in the substantia nigra die, the dopamine input to the striatum is disrupted and the entire circuit is compromised. As we will see, many therapies are targeted at preserving dopamine activity at the striatum. Surgical interventions are focused on other regions of the basal ganglia.
Causes
Despite a large amount of research on various aspects of the disease, the precise cause of Parkinson’s disease is unknown. While there have been some cases of Parkinson’s disease that have been the direct result of certain toxins, the vast majority of Parkinson’s disease cases apparently occurs spontaneously and without an identifiable cause. Cases of Parkinson’s disease without an identifiable cause are referred to as idiopathic. The disease is likely caused by a complex interplay of genetic and environmental factors. Leading theories of the cause of Parkinson’s disease include exposure to one or more substances in a person that has a genetic predisposition to the disease. Epidemiological studies have identified several regions that have higher numbers of cases of Parkinson’s disease compared to the general population. Exposure to these agents increases the likelihood of developing Parkinson’s disease. These environmental risk factors include contact or ingestion of pesticides or herbicides, living in a rural setting and the consumption of well water, and living near processing plants, certain industries and mining operations. Relatively large numbers of Parkinson’s disease cases have occurred among people in certain professions. For example, those that have had long term exposure to manganese through mining are much more likely to develop Parkinson’s disease (or a disease that is clinically indistinguishable from idiopathic Parkinson’s disease). While several agents have been identified as possible causes of idiopathic Parkinson’s disease, no one agent has been linked to all cases of Parkinson’s disease.
Our understanding of the possible causes of Parkinson’s disease and human basal ganglia circuitry in general was enhanced by an unfortunate and unlikely population of people in the 1980’s. A group of heroin-addicted men decided to inject themselves with a synthetic form of heroin which, at the time, was not illegal. The drug that they were attempting to abuse was called MPPP (1-methyl-4-phenyl-4-propionoxypiperidine) which is similar to Demerol (meperidine). Since the makers of the drug were obviously not adhering to strict quality control standards, a side product of the synthesis of MPPP was formed called MPTP (1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine). This simple decarboxylation (Figure) led to the formation of a precursor of a potent neurotoxin.
Those who injected self-administered MPTP suffered first from severe hallucinations and, within a few days, a syndrome clinically identical to advanced Parkinson’s disease. Upon close study and the help of animal models, it was found that MPTP readily crosses the blood-brain-barrier and is converted to a substance called MPP+ or 1-methyl-4-phenylpyridinium. The dopamine reuptake transporter is particularly fond of MPP+ and concentrates this compound within dopamine neurons. Once inside, MPP+ is toxic to mitochondria and poisons the energy system of the cell, causing the neurons to degenerate. Thus people who were attempting to use a designer form of Demerol instead injected a substance that selectively destroyed dopamine cells within the substantia nigra and caused a rapid transition into Parkinson’s disease.
This event led to the use of MPTP as a model for Parkinson’s disease and has lead to many discoveries about the disease and about the brain’s dopamine system in general. Injection of monkeys with MPTP creates many of the motor features of Parkinson’s disease which can be corrected with the administration of drugs. Thus MPTP has become one of the models by which new Parkinson’s disease drugs are tested in animals before they are brought to market. This model had also been used to study surgical correction of the disease as well as stem cell treatments.
It has been argued that Parkinson’s disease might actually be caused by the long term ingestion of MPTP from the environment. While levels might not be detectable, over time the levels might build up in brain to cause the disease. MPTP has also been used as a model to study the pathophysiology of Parkinson’s disease however there are certain limitations to this approach. For example, MPTP administration does not cause the formation of Lewy bodies. Lewy bodies are aberrant proteins that are invariably seen in the brains of Parkinson’s disease patients. While MPTP is extremely useful for identifying treatments for Parkinson’s disease symptoms, however MPTP alone is not sufficient as the cause of Parkinson’s disease.
More recently, another agent was shown to cause Parkinsonism in laboratory animals. In contrast to MPTP, the pesticide/herbicide rotenone not only led to selective degeneration of dopamine containing neurons, but it also creates intracellular inclusions similar to the Lewy bodies seen in Parkinson’s disease. Thus rotenone has become a compound that is closely studied as a model of Parkinson’s disease in animals. This tool allows for the creation of animals with a disease very similar to Parkinson’s disease that can be used to test drugs that correct movement disorders but also to stop or reverse the disease.
Genetics does play some role in the disease but it may not be very prominent. About five to ten percent of the time, patients with Parkinson’s disease will have had a family member with the disease. Also, when twins are studied (two individuals with the same genetic makeup), if one twin has the disease before age 50, the other twin is more likely than most to get the disease. Despite this link less than one percent of Parkinson’s disease cases can be clearly demonstrated as being directly inherited. While there is likely a genetic predisposition to Parkinson’s disease in some people, whether or not a person ultimately has the disease is based on factors other than genetics.
One gene that has been linked to an inherited form of Parkinson’s disease is the gene that codes for the parkin protein which is sometimes refered to as the PARK2 gene or simply the Parkin gene. In the small number of cases that are inherited, aberrant forms of the gene have been described. Mutations in the parkin gene lead to a very specific form of Parkinson’s disease called autosomal recessive juvenile parkinsonism. Efforts to determine if this gene is abnormal in idiopathic Parkinson’s disease have not yet shown positive results. Other identified genes that may play a role in Parkinson’s disease are alpha-synuclein, PTEN induced Putative Kinase 1, DJ-1, Leucine Rich Repeat Kinase 2 and ATP13A2. The genetic basis of Parkinson’s disease remains an area of much research interest.
Differential Diagnosis
Many diseases can cause symptoms that are similar to Parkinson’s disease and, with the lack of a definitive laboratory or radiologic test, Parkinson’s disease needs to be differentiated from other diseases based on clinical features (Table 1). In addition to various toxins and drugs that can cause parkinsonian effects, there is considerable overlap among the Parkinson-like diseases. Even within the field of movement disorders there is controversy as to the proper classification of various illnesses.
Table 1 – Differential Diagnosis in Parkinson’s Disease |
|
Alzheimer’s disease |
Medication-induced Parkinsonianism |
Cerebrovascular accident |
Multiple System Atrophy |
Corticobasal Degeneration |
Normal Pressure Hydrocephalus |
Essential Tremor |
Posttraumatic Parkisonism |
Hallervorden-Spatz syndrome |
Prion diseases |
Infectious or structural etiologies |
Progressive Supranuclear Palsy |
Lacunar syndromes |
Striatonigral Degeneration |
Lewy Body Dementia |
Toxin poisoning (manganese, methanol, MPTP, etc.) |
Clues to differentiate Parkinson’s disease from other disorders include age at symptom onset, unilateral presentation of tremor, a constellation of related symptoms, and success of dopaminergic medications. Patients that present with an atypical clinical picture should be evaluated for related diseases. For example, patients that present with tremor prior to the age of 40 should be screened for toxins and heavy metals in additional to a full physical workup. Wilson’s disease, that is, a disease in which pathological levels of copper accumulate in the body can sometimes cause tremor as its first clinical manifestation. A unilateral resting tremor at initial presentation is likely Parkinson’s disease. If the tremor began in both upper extremities simultaneously, essential tremor is the more likely diagnosis. Early in the course of Parkinson’s disease, dementia should not be present. While dementia often occurs in Parkinson’s disease later in the disease, if it coincides with tremor onset, Dementia with Lewy Bodies may be a more appropriate diagnosis.
Treatments
Medications
There are several types of medications that are used to treat Parkinson’s disease. Many of them work by increasing dopamine levels in the brain or by augmenting neurotransmission at dopamine nerve terminals. A stylized rendition of a dopamine nerve terminal and the location of action of some Parkinson’s disease drugs are shown in Figure 2. In addition to drugs that act on the dopamine system, there are agents that focus on acetylcholinergic neurotransmission. Both dopaminergic and cholinergic medications are used primarily for symptomatic relief of the movement disorder components of Parkinson’s disease. While there has been some suggestion that levodopa may slow down the progression of the disease, the medicines currently approved for treatment are for symptomatic relief. That means that the cells in the brain continue to die of time. There is no cure for Parkinson’s disease and no drug exists right now that can arrest or reverse the destruction of neurons.
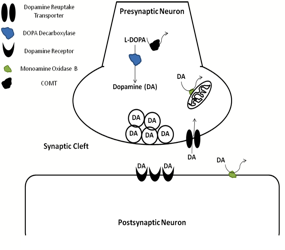
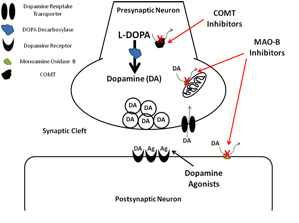
Figure 2 – CNS Dopaminergic Nerve Terminal and Effects of Parkinson’s Disease Drugs
The top panel graphically depicts a synaptic cleft at a nerve terminal of a dopamine neuron. L-DOPA is converted to dopamine (DA) in the nerve terminals by an enzyme called DOPA decarboxylase. The DA is held in synaptic vesicles until it is released. The DA interacts with DA receptors on the postsynaptic neuron. DA is removed from the synaptic cleft by diffusion or through reuptake by transporter molecules in the membrane of the presynaptic terminal. DA is also degraded by catechol-O-methyl transferase (COMT) and monoamine oxidase B (MAO-B).
The bottom panel shows the locations of various drugs used in PD. Levodopa or L-DOPA supplied exogenously will increase the synthesis of DA. MAO-B inhibitors and COMT inhibitors block the degradation of DA. DA agonists act directly on DA receptors and stimulate postsynaptic cells.
Levodopa/Carbidopa
Since Parkinson’s disease is a disease that results in the destruction of dopamine-containing neurons in the brain, one goal of therapy has been to provide additional dopamine to the brain. Unfortunately, dopamine by itself cannot cross the blood-brain barrier. Also, even very low levels of dopamine can have profound effects on blood pressure such that dopamine is often used as a pressor in intensive care units. One way to get over these two therapeutic hurdles is to administer the precursor to dopamine, or DOPA. Levodopa or L-DOPA can cross the blood-brain barrier and is made into dopamine by the enzymatic action of DOPA decarboxylase in nerve terminals (Figure 2). As it so happens, L-DOPA is also converted to dopamine in areas other than brain. Thus giving levodopa by itself results not only in increased levels of brain dopamine but also in the periphery, which could be harmful if it was converted to dopamine. Because of this, levodopa is always administered with another drug, carbidopa. Carbidopa blocks DOPA decarboxylase but does not cross the blood-brain barrier. Therefore when levodopa/carbidopa is given to patients, the levodopa enters the brain to create more dopamine in nerve terminals but carbidopa blocks levodopa’s effects in the rest of the body. The combination of these two agents is the mainstay of Parkinson’s disease treatment and has been used with great success for decades. Arvid Carlsson won the Nobel Prize in Physiology or Medicine in 2000 for his work in this area during the 1950s.
Levodopa/carbidopa is marketed under the brand name Sinemet or Atamet. Over time, levodopa/carbidopa tends to become less useful. As the disease progresses and there are fewer dopamine-containing nerve terminals, the dose of levodopa must be increased to utilize the enzymatic machinery in the few remaining cells. Unfortunately, as the usefulness of the drug begins to decrease, the chance of side effects increases thus, the therapeutic window decreases.
Monoamine Oxidase Type B Inhibitors
Dopamine neurons originating in the substantia nigra and terminating in the striatum are destroyed in Parkinson’s disease. The motor symptoms of Parkinson’s disease do not develop until a majority of cells have been destroyed. One goal of therapy is to increase the amount of dopamine that is present at nerve terminals located in the striatum. A way to achieve this is to block the degradation of dopamine into other compounds. Since monoamine oxidase type B (MAO-B) is an enzyme that is able to metabolize dopamine, a group of medications that inhibit MAO-B can keep dopamine levels up in brain (Figure 2). The prototypical MAO-B inhibitor in this class is selegiline (L-deprenyl; Eldepryl, Atapryl, Carbex, others). By blocking an enzyme that breaks down dopamine, more of this neurotransmitter is available to act on the striatum and keep the basal ganglia circuitry in order. Newer MAO-B inhibitors include Azilect (Rasagiline) which binds irreversibly to MAO-B and blocks its action on dopamine. Newer agents appear to have fewer side effects than older drugs.
The primary side effect of MAO-B inhibitors are that can cause symptoms consistent with an overabundance of dopamine including hallucinations, increased motor activity, nausea and flushing. MAO inhibitors can interact with a number other drugs and they need to be used with caution. Use of these agents with Demerol (meperidine), other opioids, selective serotonin reuptake inhibitors, and tricyclic antidepressants can lead to severe agitation, muscle rigidity and even death. As with all medications for Parkinson’s disease, MAO-B use should be coordinated by a neurologist, preferably one with specialized training in movement disorders. All medicines, including those used for Parkinson’s disease, should be considered before starting a new treatment. Also, MAO-B inhibitors should not be stopped abruptly except in cases of severe side effect.
Catechol-O-Methyl Transferase (COMT) Inhibitors
Catechol-O-methyl transferase (COMT) inhibitors (Comtan, Tasmar) improve dopamine neurotransmission in a slightly different way. Instead of blocking the enzyme that breaks down dopamine, COMT inhibitors block the degradation of L-DOPA (Figure 2). Since L-DOPA is the immediate precursor to dopamine, COMT inhibitors promote increased dopamine synthesis by preventing L-DOPA breakdown. One of these agents would be used to improve or sustain the action of levodopa/carbidopa. In fact, medicines like Comtan are only approved for use in conjunction with levodopa/carbidopa. As was mentioned, over time, the therapeutic window for levodopa decreases and the symptoms of Parkinson’s disease tend to return in between doses. COMT inhibitors are used in cases where patients observe a return of symptoms at the end of each dose.
Side effects of COMT inhibitors may occur and include diarrhea, increased motor activity, nausea, fatigue and hallucinations. In some cases COMT inhibitors may cause orthostatic hypotension i.e. a sudden drop in blood pressure when the patient rises from a sitting or laying position. Rarely, these agents may cause rhabdomyolysis (muscle breakdown) or neuroleptic malignant syndrome.
Dopamine Receptor Agonists
Another way to compensate for the decrease in dopamine nerve terminals in the striatum are by using dopamine receptor agonists (bromocriptine [Parlodel®]; pergolide [Permax®]; pramipexole [Mirapex®]; ropinirole [Requip®]; apomorphine [Apokyn®]; others. Since dopamine-containing cells from the substantia nigra preferentially die in Parkinson’s disease, the total amount of dopamine acting on postsynaptic neurons in the striatum (their target) is decreased. Dopamine binds to and stimulates dopamine receptors on neurons in the striatum (Figure 2). Dopamine agonists are molecules that can cross the blood-brain-barrier, bind to and stimulate dopamine receptors.
While attempts have been made create dopamine receptor agonists that are selective for dopamine receptors only in the striatum, there is some overlap, especially at higher doses. Thus when dopamine receptor agonists are administered they may stimulate any cell in the body that contains dopamine receptors. This binding explains most of the side effect profile of dopamine receptor agonists. Side effects include drowsiness, nausea, and orthostatic hypotension. Some of the more serious or disturbing side effects are confusion, hallucinations, and psychosis.
Amantadine
Amantadine (Symmetrel®) is used in idiopathic Parkinson’s disease, postencephalitic Parkinsonism and the symptoms of Parkinson’s that occur after toxins (such as carbon monoxide). Amantadine was first used as an antiviral agent and was shown to be effective in the treatment of symptoms of Parkinson’s disease. Despite being used as an anti-Parkinson’s disease drug for many years, the exact mechanism of action is still not known. It was originally thought to affect dopamine neurons but more recent evidence suggests that it is a weak, non-competitive antagonist of the NMDA glutamate receptor. It also causes anticholinergic side effects which are not explained by receptor binding. Amantadine is used
Once a stable regimen has been established, amantadine must not be stopped abruptly as a rapid clinical deterioration may occur (Symmetrel prescribing information, Endo Laboratories, July 2002). The most common side effects are nausea, dizziness and insomnia. Amantadine may also cause hallucinations, ataxia, headache, abnormal dreams, diarrhea and agitation. This drug should not be given to patients with untreated glaucoma. Amantadine may also exacerbate congestive heart failure and lead to peripheral edema. Finally, amantadine is associated with livedo reticularis which is a purple mottling of the skin, usually on the legs. While it is not inherently serious, is can be disconcerting to patients.
Anticholinergic Medications
Anticholinergics were among the first drugs used to treat Parkinson’s disease but their use has declined with the advent of drugs that target the dopamine system directly. Nevertheless, anticholinergic agents remain a useful adjunct to dopaminergic therapy in Parkinson’s disease. Some of the more commonly used anticholinergics used in Parkinson’s disease are biperiden HCL (Akineton®), benztropine mesylate (Cogentin®), procyclidine (Kemadrin®) and trihexyphenidyl (Artane®). It is not known precisely why anticholinergics are of benefit in Parkinson’s disease but the leading theory is that dopaminergic and cholinergic pathways counterbalance one another in the basal ganglia. As nigrostriatal neurons die in Parkinson’s disease, the cholinergic processes dominate. Therefore since the dopamine circuits are being corrupted by the disease and leading to motor effects, anticholinergic agents reign in the overactive cholinergic system.
As expected, the major side effects of anticholinergic agents are anticholinergic effects such as dry mouth, blurry vision, sedation, delirium, constipation and urinary constipation. As the cholinergic circuits are dampened by anticholinergics, the dopamine system may become overactive and these agents may be associated with confusions and hallucinations.
Disease-Modifying Agents
The medicines that are commonly used to treat Parkinson’s disease improve the symptoms (mainly motor symptoms) of the disease. Since Parkinson’s disease is a progressive neurodegenerative illness, at a certain point in the progression of the disease, drugs that only treat the symptoms or Parkinson’s disease will no longer be effective. An active area of research is to identify drugs that prevent dopamine neurons from dying at all. These drugs are sometimes referred to as disease-modifying drugs. Many of these agents are still in the clinical trial stage and their efficacy and safety have yet to be determined. The hope is that by blocking neuronal cell death that Parkinson’s disease can be cured or at least the progression of the disease can be slowed.
One of the first disease-modifying agents to be tried and shown to be at least somewhat effective is coenzyme Q-10. This drug is something that is found naturally in cells and is related to mitochondria, the power plants of cells. The amount of coenzyme Q-10 in the body and brain decreases with age. In those that are deficient, coenzyme Q-10 supplementation as been shown to be effective. It has also been demonstrated in certain studies that coenzyme Q-10 supplementation may help to treat certain diseases such as high blood pressure (best evidence) and even Parkinson’s disease as well as others. Clinical trials are ongoing but it appears that coenzyme Q-10 is only modestly able to the progression of Parkinson’s disease. In fact some researchers argue that the benefit of coenzyme Q-10 supplementation is solely on symptoms rather than on nerve cell death. In any case, coenzyme Q-10 is very well tolerated and very safe. Even if it results in only modest benefit in Parkinson’s disease, larger trials may argue for its use as an adjunct therapy in all patients with Parkinson’s disease.
Eliprodil is an antagonist at the NMDA glutamate receptor and is possibly neuroprotective in Parkinson’s disease. Excessive stimulation of NMDA receptors can lead to excitotoxic cell death in neurons and may play a role in the pathology seen in Parkinson’s disease. This agent was shown to be effective in treating primates that had been given MPTP. A phase II trial has recently been completed to assess eliprodil and the results have yet to be published.
Another putative agent that has been progressing through clinical trials is talampanel or LY300164. This drugs may exert a neuroprotective benefit by blocking AMPA receptors, another major type of glutmate receptor in the brain. This agent has recently completed Phase II trials.
In addition to treatments that block glutamate receptor activity, other possible neuroprotective agents include antioxidants and free-radical scavengers. These drugs are known to protect dopamine cells from degenerating in a dish and may work within brain. Studies looking at these agents are ongoing.
Surgery
Ablation or Destructive Therapy
The two main “destructive” therapies that are available to patients with Parkinson’s disease are thalamotomy and pallidotomy. Considering the anatomy of the basal ganglia (Figure 1) and the effect that a loss of dopamine neurons have on the motor system, there are two main areas that could be ablated or destroyed in order to improve function. Prior to levodopa/carbidopa treatment, destruction of a part of the thalamus called the ventral intermediate nucleus was the primary treatment in Parkinson’s disease. An early variation of this surgery was routinely performed as early as the late 1940s and is/was very effective at relieving the tremor associated with Parkinson’s disease. Unfortunately it has not always effective in treating other symptoms of Parkinson’s disease and is used only in cases that are refractory to other treatments. The surgical procedure that is most often performed in patients with advanced Parkinson’s disease is a pallidotomy. By lesioning a specific part of the globus pallidus interna (the posteroventral portion) and part of the subthalamic nucleus, Parkinson’s disease patients show benefits in rigidity, tremor and bradykinesia. While there is some argument that the improvement of tremor is better with thalamotomy rather than pallidotomy, the improvement in all symptoms cannot be ignored. Pallidotomy has lead to a 90 percent improvement of the bradykinesia scores on the Unified Parkinson's Disease Rating Scale (UPDRS) even at two years after the surgery.
Deep Brain Stimulation
The newest and increasingly becoming the most common surgery for Parkinson’s disease is deep brain stimulation. This procedure involves neurosurgeon implanting thin electrodes deep within the brain so that small electrical impulses can be delivered to areas of the basal ganglia. Where ablation surgery destroys areas of the basal ganglia that are overactive, deep brain stimulation stimulates areas of the basal ganglia that are hypoactive or overly inhibited. The major advantages to deep brain stimulation versus ablation are that the former is reversible, adjustable and is safer than destructive techniques. The stimulator can be adjusted remotely in order to provide just enough stimulation to overcome symptoms.
There are three main locations in the basal ganglia that are target for deep brain stimulation: the ventral thalamic nuclei, the globus pallidus interna and the subthalamic nucleus. The choice of location is complex but is roughly chosen by symptoms and relative response to therapy. Implantation into the ventral thalamic nuclei is performed primarily to treat tremor and is effective in over 80 percent of patients. The globus pallidus interna is chosen when treatment is aimed at correcting bradykinesia, gait and speech disturbances and drug-induced dyskinesias (movement abnormalities). The newer and apparently more broadly effective procedure is deep brain stimulation of the subthalamic nucleus. Improvements have been seen in bradykinesia, rigidity, tremor, and in gait and posture. The procedure is very safe, is not associated with operative mortality and does not seem to contribute to psychiatric conditions as has been reported with other types of deep brain stimulation. One curious case report details a link between spontaneous pathologic gambling and bilateral (both sides) subthalamic nucleus deep brain stimulation. It is important to note that while deep brain stimulation improves quality of life, it has not been shown delay overall mortality.
Neuronal Cell Transplant
It seems reasonable that since dopamine-containing neurons are being lost in the substantia nigra that one therapeutic strategy would be to surgically insert new dopamine neurons into the brain. Cells from several sources have been tried.
Since the medulla of the adrenal gland contains dopamine secreting cells, Parkinson’s disease patients have undergone surgery to remove part of the adrenal gland and have it placed near the substantia nigra. This surgery is not often performed because of the high complication rate of the surgery. Surprisingly, the dangerous part of the surgery is not the insertion into the brain, but the high complication rate associated with disrupting the adrenal gland.
Xenografts are tissue or organs harvested from animals other than humans are transplanted into humans. Tissue harvested by the brain of fetal animals has been used to attempt to replace the substantia nigra. Because of various similarities to humans, fetal pigs are currently the leading source xenografts for Parkinson’s disease surgery. This approach is currently in clinical trials.
Fetal cells have also been harvested from human embryos for use in Parkinson’s disease patients. Also, stem cells from aborted fetuses have been used to replace areas dopamine-containing cells. Both of these approaches are mired in controversy and advancements in this area are difficult. Of the limited number of studies that have been performed, mostly in countries outside of the United States, embryonic stem cells appear to significantly reduce symptoms although it is too soon to determine if they can halt the disease completely. As of March 2009, the presidential order banning stem cell research has been lifted. Research in this area will undoubtedly progress more rapidly and new results are forthcoming.
Rehabilitation
Physical, occupational and speech therapy all have a place in Parkinson’s disease. The long term benefits of each are difficult to assess because the disease is variable and progressive. However, employing rehab services early and occasionally throughout the course of the disease improves quality of life. Physical therapy may not change the course of Parkinson’s disease by exercises that seek to improve range of motion, postural control, endurance and mobility may help to improve symptoms of the disease. Because certain muscle groups are not routinely activated, they can lose conditioning. Over time, even as motor programs are executed the muscle tone may not be present to carry out the neural order. Physical therapy can keep these muscles conditioned.
Occupational therapy aims to improve upper limb dexterity including fine motor skills. With tremor and rigidity, these skills may become compromised early in Parkinson’s disease. Occupational therapists can identify areas of particular weakness and develop strategies and tools to deall with functional deficits.
Troubles with swallowing are common in Parkinson’s disease. Speech therapy may not be called upon as often as necessary in the treatment of patients with Parkinson’s disease. It is important to routinely test swallowing and gag reflex for functional decline. Also, as hypophonia is a common problem, speech therapists can attend to breath control, rate control, articulation and volume.
Recreational therapists can greatly improve quality of life for patients and ther families. They are creative resources for identifying disease-appropriate recreational activities that can be enjoyed by all members of the caregiving structure. Proper recreation can help combat the isolation and detachment that patient’s with Parkinson’s disease often experience.
Disease Severity and Course
Parkinson’s disease is a progressive neurodegenerative disease that currently has no cure. As clinicians treat patients with the disease and researchers attempt to find new ways to combat the illness, it has been useful to create standardized tools for assessing the level of function and disability in Parkinson’s disease patients. Several scales have been developed, each of differing complexity, which have attempting to capture all of the features of the disease. These scales help physicians monitor the effect of treatments on their patients and, unfortunately, also plot the course of their decline. These tests also provide a common scale by which treatments can be discussed across different studies. While there are limitations, using standardized scales allows one to compare the effect of a surgery done recently with a drug effect seen years ago. As you might expect, those scales with more questions are more accurate and provide a wealth of information, but they are also very time consuming. Each scale and sometimes a combination of scales are used, depending on the purpose. The scales listed here are the most commonly used and are often seen in patient records and in research done in the area of Parkinson’s disease.
Unified Parkinson's Disease Rating Scale (UPDRS)
The Parkinson’s disease is a rating tool to follow the longitudinal course of Parkinson's Disease (Appendix). Given its complexity, it is usually reserved for clinical trials and scientific studies. The score is determined during interview and physical exam. A maximum of 199 points are possible and a score of this magnitude would indicate total disability. A score of zero indicates no disability though it is unlikely to find a patient with Parkinson’s disease that will score either 199 or zero. Medications should lower a patient’s UPDRS score, at least temporarily. If they live long enough, patients with Parkinson’s disease will experience worsening symptoms and increasing UPDRS scores. The UPDRS, or a portion of it, is routinely used as a means of patient evaluation in treatment protocols and to make correlation neuroradiographic changes. The UPDRS is occasionally refined to improve usefulness and precision (Geotz et al., 2008).
Hoehn and Yahr Staging
For most applications, the rating scale developed by Hoehn and Yahr in 1967 is both practical and time effective (Table 2). Given its lack of detail, the Hoehn and Yahr staging may not be ideally suited to many treatment study paradigms, although it is still used (Morris, et al., 2009). While it does not provide the level of detail of the UPDRS, it is a useful tool to track disease progression at clinical appointments. Patients with Parkinson’s disease progress to higher stages of the Hoehn and Yahr scale in a predictable fashion. It has been suggested that patient’s with typical idiopathic Parkinson’s disease will advance from one stage to the next in two to three years (Marttila & Rinne, 1977) more recent studies suggest that with optimal treatment that patients progress between stages every 3.5 to 7 years (Hely et al., 1999).
Table 2 –Hoehn and Yahr Staging for Parkinson’s Disease |
|
Stage One
|
Signs and symptoms on one side only |
Stage Two |
Symptoms are bilateral |
Stage Three |
Significant slowing of body movements |
Stage Four |
Severe symptoms |
Stage Five |
Cachectic |
Schwab and England Activities of Daily Living
Third Parkinson’s disease rating scale that is commonly used to track the progress or deterioration of function in patients with Parkinson’s disease is the Schwab and England Activities of Daily Living Scale (Gillingham & Donaldson, 1969). As the name implies, this rating scale determines functional capacity by assessing function based on the degree to which a Parkinson’s disease can perform that skills necessary to survive. For the top three of the levels, the patient is still considered fully independent though they may take significantly longer to complete activities than would a healthy person of the same age. Of note, these ADLs are different than the basic and instrumental ADLs commonly used by nurses and occupational therapists.
Table 3 - Schwab and England Activities of Daily Living |
100% - Completely independent. Able to do all chores without slowness, difficulty or impairment. Essentially normal. Unaware of any difficulty. |
90% - Completely independent. Able to do all chores with some degree of slowness, difficulty and impairment. Might take twice as long. Beginning to be aware of difficulty. |
80% - Completely independent in most chores. Takes twice as long. Conscious of difficulty and slowness. |
70% - Not completely independent. More difficulty with some chores. Three to four times as long in some. Must spend a large part of the day with chores. |
60% - Some dependency. Can do most chores, but exceedingly slowly and with much effort. Errors; some impossible. |
50% - More dependent. Help with half, slower, etc. Difficulty with everything. |
40% - Very dependent. Can assist with all chores, but few alone. |
30% - With effort, now and then does a few chores alone or begins alone. Much help needed. |
20% - Nothing alone. Can be a slight help with some chores. Severe invalid. |
10% - Totally dependent, helpless. Complete invalid. |
Diet and Nutrition
Gastrointestinal dysfunction is one of the most common consequences of Parkinson’s disease aside from classic motor and behavioral issues (Pfeiffer, 2003). Constipation and other difficulties with bowel motility can become create significant challenges for patients with Parkinson’s disease. While it is not uncommon for bowel motility to decrease with age, Parkinson’s disease is thought to directly affect the enteric nervous system and slow the movement of fecal material through the GI tract. From the early stages of the disease, it is important to maintain a diet high in fiber. Fiber acts as a bulk-forming laxative to improve the motility of the bowel. As the disease progresses and fiber alone is not sufficient to ensure gastric and bowel motility, a primary care physician or gastroenterologist should be consulted.
Stages of Grief
The diagnosis of Parkinson’s disease has a profound impact on patients and their families. For diseases in which there is no cure, such as Parkinson’s disease, many of those touched by the disease go through stages of grief, similar to the Kübler-Ross model. The five basic stages of this process are denial, anger, bargaining, depression and acceptance. The speed at which patients (and even caregivers) move through this process can influence the course of the disease. Patients that have not yet reached the acceptance stage are very difficult to manage and treat. Identifying a patient’s stage of grief about this illness can aid in attempts to treat the disease from medical, social and occupational perspectives.
The first stage of the process, denial, is often a significant barrier early in the disease. It usually starts before the diagnosis of Parkinson’s disease is even made, when motor difficulty in an arm is repeatedly overlooked as clumsiness. Also, once the diagnosis is made, patients and caregivers may seek out additional medical opinions. Denial can result in a patient refusing to tell others about the disease, missing appointments, and neglecting to take prescribed medicines.
Anger can be particularly damaging to families and ultimately very harmful to the long term outcome of the patient. It is impossible to predict with any certainty how people will react to the diagnosis of a progressive, neurodegenerative disease; however, anger often plays a role, even for a brief time. The psychological reaction to the diagnosis may leave patient’s feeling that life is not fair or asking “why me?” Caregivers may be angry as well, perhaps not with the patient, but with the circumstances of life in general. These issues of anger need to be identified and dealt with fully before the patient with Parkinson’s disease exhibits a significant drop in ADLs. He or she will become increasingly dependent as the disease progresses and a strong support system is vital to the wellbeing of both patient and caregiver. To this end, the psychological status of the caregiver needs to be routinely evaluated and support should be given whenever possible.
Patients and families often adopt bargaining strategies when presented with treatment options. Since Parkinson’s disease is a disease with no cure, it is common for lifelong consumers of Western Medicine to ask if there are clinical trials or experimental therapies that could be implemented. While it certainly reasonable to discuss the role of clinical trials in a patient’s care, a realistic assessment of the disease course and existing treatment options should always be given. There is in an inherent power in optimism when it comes to disease, however optimism should not interfere with the administration of currently available therapies. Most importantly, hope in experimental or more exotic treatments should not stand in the way of patient and family education. While the line between hope and avoidance becomes difficult to detect in the course of Parkinson’s disease, if a patient refuses to learn about the disease because all hopes are pinned to a future cure, expectations should be readjusted.
Depression is a particularly difficult stage in the grieving process and may be a direct consequence of the disease. Estimates of the prevalence of depression in Parkinson’s disease are approximately 40% (Slaughter et al., 2001). While it is true that facial expression does not indicate mood in patients with Parkinson’s disease (i.e. “masked facies” are a symptom of the disease and do not represent the true emotional state of the patient), the decreased motor activity in the face may lead physicians and other health care providers to overlook the diagnosis of depression.
Work and Life Adjustments
Parkinson’s disease can strike before people have hit retirement age, and often does. Early in the disease it may be possible to extend a patients ability to work for several years. If a job requires manual dexterity, it may be unlikely that a person with Parkinson’s disease can maintain that job indefinately. Even jobs that require less motor control may become too challenging as the disease progresses. It is important that patient’s and families are optimistic yet realistic when it comes to Parkinson’s disease at work. While medication can stop many of the motor issues of Parkinson’s disease for years, this time may be suited in making preparations for a life after work. Understand that overmedication early in the disease may mean that treatment later in the disease course may not be possible. If one uses medication to perform the increasingly challenging demands of work early in the disease, the price may be that the drugs no longer work later in the illness.
Telling an employer about a diagnosis of Parkinson’s disease is highly personal and needs to be carefully considered. The reaction of an employer is difficult to gauge ahead of time and needs to be anticipated as much as possible. On the one hand, certain allowances can be made to Parkinson’s disease patients without harming productivity. Perhaps certain job functions that are more difficult with decreased motor function can be traded off for others that are less physically demanding. Perhaps a flexible schedule can be implemented that will allow for a midday nap with the concession that an extra hour be worked in the morning or the evening. Some employers may not make any allowances for individuals with Parkinson’s disease and may even subtly discriminate against them.
Promotions, work details, incentives and other perks of the job may not be open once someone declares that diagnosis. If motor disturbances of the disease interfere with safety at work, it becomes more imperative to discuss the diagnosis with management. Certain allowances must be made according to federal and state guidelines, but, as often happens when no one is around to enforce them, certain allowances may not be made immediately or at all. Therefore it is important to know employee rights but also to be aware that having them realized may require a bit of effort.
It is important to recognize that even with treatment certain activities that were once enjoyable may not be available to the patient. For example if the person used to enjoy a hobby that required a high degree of manual dexterity, like model building or playing an instrument, it may not be possible continue that hobby in the same way it was enjoyed previously. One way work with this problem is by continuing to stay involved in the area and not to leave it totally. Perhaps the person could teach others how to perform a certain task, not by showing, but by saying. In that way the patient continues to experience the joy of the hobby but also can enjoy the satisfaction of passing knowledge on to others. It is also very important to maintain some role in activities that were shared between married couples when one has the disease. Part of the identity of that relationship is defined by the experiences that are shared. Great effort should be devoted to maintaining this connection as much as possible with an awareness that certain things will no longer be possible as the disease progresses. New experiences, ones that are physically possible in Parkinson’s disease, should slowly supplant the old experiences. However, old memories should be relished as new ones are being formed.
As was mentioned, dementia occurs all too frequently in Parkinson’s disease. Certain memory devices should be instituted before memory begins to fail. There is comfort in routines but they also help to prevent losing key things, forgetting key pieces of information and help to maintain a sense of control. Use routines when they are of benefit but avoid them if they prevent experiencing certain aspects of life that require new experiences, especially ones that are available to those with a motor disability.
An open dialogue must be maintained between the patient with PD and their spouse or primary caregiver. Expectations about the disease and the couple’s life need to be expressed, understood and accommodated as much as possible. It is important to understand what things can be changed and what things cannot. Questions need to be raised when they are an issue, even if they are sensitive. Patients may not also talk about their sexual life to a medical professional so the onus is on the professional to engage in that discussion even if it may seem awkward. Parkinson’s disease may affect sexual relations in a way that can be treated medically or through counseling. Other issues need to be identified and addressed before they become major problems. Often times it is the medical professional that must ask the questions that have not be mentioned and ask if certain things are alright, even if they are not mentioned by the patient or the caregiver. Assuming that everything is fine when it is likely not perpetuates problems and worsens the quality of life for patient’s with Parkinson’s disease and their caregivers.
Counseling
Parkinson's disease, as with many chronic illnesses, effects both physically and mentally. It is important for the patient to realize that they are not alone.
The decision to seek counseling is an important step. Too often, people don't get help because they feel guilt, shame, or embarrassment.
The biochemical changes occurring in the brain with Parkinson's disease can lead to depression. Depression is a real part of the disease as much as tremor or slowness of movement. In some people, medical treatment of the depression is necessary.
An assessment is used to diagnose the problem and determine the best treatment. The assessment starts by asking the client to describe any symptoms they have had (emotional, mental, and physical) and a medical history is taken. A question-and-answer survey is also given to assess the client.
Once the assessment is complete, a treatment plan can be chosen. At this time, you can discuss with the client:
- The best type of counseling
- The best setting for counseling (counselor's office, outpatient clinic, hospital, residential treatment center)
- Who will be included in the treatment (cleint, family members, others with similar problems)
- How often counseling sessions are needed
- How long counseling may last
- Any medications that will be needed
What Types of Counseling Are Available?
The following list briefly describes common types of counseling. These can be used together or alone, depending on your treatment plan.
Crisis intervention counseling. In cases of emergency (such as initial despair over diagnosis), the counselor will help the client get through the crisis and refer them to further counseling or medical care, if needed. These services are provided by community health agencies, helplines, and hotlines.
Individual counseling. This type of counseling works well when problems come mainly from the clients thinking patterns and behaviors. Also, some problems are very personal and difficult to confront with others present. If the client is experiencing depression, anxiety or grief in dealing with Parkinson's this type of counseling may be appropriate.
Family therapy. A diagnosis of Parkinson's disease can affect the entire family. If the client is the primary provider in the home, there can be financial strain. If the client is the homemaker, there may need to be adjustments in the distribution of chores. These everyday strains combined with the emotional effects of dealing with a chronic illness have an enormous impact on the family dynamic.
Family therapy can help family members resolve issues among each other. It can also help them adopt ways to help another family member cope better. Family members can learn how actions and ways of communicating can worsen problems. With help, new and improved ways of communicating can be explored and practiced.
Group therapy. In group therapy, the client joins a group to discuss problems together. A counselor guides the session. Members in the group often share the same problem, but not always. The group session provides a place where people can confide with others who understand their struggles. They also can learn how they see themselves and how others see them. Members gain strength in knowing that they are not alone with their problems.
Residential treatment. With this type of therapy, the client lives at a treatment center. The length of stay can vary, depending on the treatment program and progress of therapy. A program can last more than a year or just a week or two. Settings include hospitals, home-like structures, and clinics.
Focus is mainly on the problems the client is experiencing and getting well. Other activities, such as work, family, and hobbies, take a backseat to treatment. In most programs, the client receives counseling daily and participates in regular group therapy. Additional counseling after residential treatment has ended may be needed.
Self-help and support groups. These include a network of people with similar problems. These groups usually meet regularly without a therapist or counselor.
Daily Activities
Parkinson’s Disease can affect many aspects of a person’s daily life. However, with careful planning and activity moderation, the effects of Parkinson’s Disease can become much less stressful and intrusive.
The following suggestions offer guidance to overcome some of the difficulties associated with Parkinson's disease.
Hand out for your clients
Daily Living with Parkinson’s
- Plan periods of rest. Be sure to get plenty of rest. You may need to plan at least one rest period every day. If you have swelling in your feet or ankles, elevate your legs when you are resting or sitting for prolonged periods. Avoid working long days. Rest between recreation and leisure activities.
- Conserve your energy. Using less energy with daily tasks can help you have more energy to do more activities during the day. You may need to cut down on some of your activities or use energy-saving devices or techniques. If daily self care or home care activities are too tiring, discuss this with your doctor.
Energy Conserving Tips
- Simplify your tasks and set realistic goals. Don't think you have to do things the same way you've always done them.
- Plan your activities (chores, exercise, and recreation) ahead of time. Space them out throughout the day. Do not schedule too many things to do in one day. Do the things that take more energy when you are feeling your best.
- If needed, rest before and after activities.
- If you become tired during an activity, stop and rest. You may need to finish it on another day or when you feel less tired.
- Do not plan activities right after a meal. Rest 20-30 minutes after each meal.
- Ask for help. Divide the tasks among family and friends.
- Get a good night's sleep and elevate your head when sleeping. Be careful not to nap too much during the day or you might not be able to sleep at night.
- If your doctor says it's ok, you may climb steps. You may need to rest part of the way if you become tired. Try to arrange your activities so you do not have to climb up and down stairs many times during the day.
- Avoid extreme physical activity. Do not push, pull or lift heavy objects (more than 10 pounds) that require you to strain.
When dressing:
- Get dressed while sitting in a chair that has armrests -- this will help you keep your balance.
- Roll from side to side to get pants over your hips. You can do this while sitting in a chair or lying down on your bed.
- Wear clothes that are loose fitting and have elastic waistbands.
- Choose wrap-around clothing instead of the pullover type. Also choose clothing that opens in the front, not the back so you don't have to reach behind you.
- Wear clothing with large, flat buttons, zippers or Velcro closures.
- Use a button hook to button clothing.
- Use a dressing stick if you have shoulder weakness to get your coat or shirt on or off.
- Use a zipper pull or attach a leather loop on the end of the zipper to zip pants or jackets.
Wear slip-on shoes or buy elastic shoelaces that allow you to slip your shoes on and off without untying the laces. Use devices such as a sock donner and long-handled shoehorn for additional assistance.
When bathing:
- Use a shower chair if necessary.
- Use a hand-held hose for showering and bathing.
- Use a long-handled sponge or scrubbing brush.
- Use soap-on-a-rope, bath mitts or sponges with soap inside or a soft soap applicator instead of bar soap.
- Use lukewarm water, as very hot water can cause fatigue.
- Sew straps on towels to make them easier to hold while drying.
- Place a non-skid rug on the floor outside the tub to dry your feet so you don't slip.
- Put a towel on the back of your chair and rub your back against it to dry. Or, use a terry cloth robe instead of a towel to dry off.
When toileting:
- If needed, use a bedside commode.
- In the bathroom, use an elevated toilet seat and/or safety rails to assist standing from a low surface.
When grooming:
- Do all of your grooming (shaving, drying your hair, etc) while sitting.
- Use hairbrushes and combs with built-up handles or handles with finger loops.
- Use toothbrushes with built-up handles or use an electric toothbrush.
When eating and drinking:
- Don't rush your meals. Allow the extra time you need to finish your meal. Rest your elbows on the table to provide more motion at your wrist and hand.
- Sit with your knees and hips bent at a 90-degree angle in a straight-back chair.
- Use utensils with built-up, lightweight handles, or use a "spork" -- a spoon and fork in one. Use a rocker knife for cutting food.
- Use a non-skid mat to stabilize objects on the table.
- Use a plate guard or plate with a raised lip to prevent food from spilling.
- Use a long straw with a non-spill cup or use a plastic mug with a large handle.
When eating and drinking:
- Don't rush your meals. Allow the extra time you need to finish your meal. Rest your elbows on the table to provide more motion at your wrist and hand.
- Sit with your knees and hips bent at a 90-degree angle in a straight-back chair.
- Use utensils with built-up, lightweight handles, or use a "spork" -- a spoon and fork in one. Use a rocker knife for cutting food.
- Use a non-skid mat to stabilize objects on the table.
- Use a plate guard or plate with a raised lip to prevent food from spilling.
- Use a long straw with a non-spill cup or use a plastic mug with a large handle.
When cooking:
- Use the back burners and keep pot handles turned inward.
To prevent drooling or salivation:
- Suck on hard candy, lozenges or gum to control excess saliva
- Use a straw when drinking to strengthen the muscles of the lips, mouth and throat.
To aid writing:
- Use large print, instead of script writing. Try using weighted pens or pencils and wrap black electrical tape around the barrel for additional grip.
- Use magic markers and large tablet on an easel.
To aid shopping:
- Call ahead to make sure the store has the item you need.
- Call ahead to reserve a wheelchair or tri-wheel cart if you aren't planning to bring your own.
- Call a taxi or ask a friend or family member to drive you.
To aid cleaning:
- Use long handles on sponge mops, cleaning brushes, dust pans, brooms or window washers.
- Sit to fold laundry, wash dishes, iron clothes, use the sweeper, mop the floor or to plug in appliances at low outlets. Adapt counters so that you can reach them from your wheelchair or from a sitting position.
To aid standing and sitting:
- Bend slowly at the waist and touch your toes before trying to rise from a seated position.
- Once standing, remain in place for a few seconds before trying to walk. This will help you regain your balance.
- Place an additional cushion or book to add height to your chairs and add firmness, this will help you to decrease the distance when sitting or standing.
- To make it easier to get out of bed, tie a sheet to the bed post and knot the other end so you can grasp the sheet to rise to a sitting position.
To ease cramps, spasms and tremors:
- Massage (or have someone else massage) your legs nightly to relieve leg cramps.
- Take warm baths and use heating pads to help relieve muscle spasms and ease cramps.
- Use mineral ice to relax sore joints and muscles.
- Squeeze a small rubber ball to reduce hand tremors.
- At first indication of a tremor, if possible, try lying on the floor, face down, and relaxing your body for 5 to 10 minutes.
To prevent freezing in place:
- Count your steps as you walk.
- Rock in place from foot to foot to get moving again.
- Have someone place their foot in front of you, or visualize something you need to step over, to get moving again.
Other helpful hints:
- Purchase a small battery-powered alarm pillbox to help you remember your medication schedule.
- Use a speaker phone or telephone headset to ease the problem of hand tremors while talking on the phone.
Install an intercom system or purchase walkie-talkies to make contact within the home easier.
If you have difficulty using writing utensils, try typing notes or letters on a computer or typewriter.
At Home With Parkinson's: Adapting Your Environment
Effects from Parkinson’s disease, such as fatigue and difficulties getting around, can make activities of daily living -- including leisure activities -- more difficult for people with Parkinson's disease. The following tips will help you learn to function independently and successfully in your home.
Fatigue and difficulties getting around can make activities of daily living -- including leisure activities -- more difficult for people with Parkinson's disease. The following tips will help you learn to function independently and successfully in your home.
General Safety Guidelines:
- Have emergency numbers (police, fire, poison control, and a neighbor's phone number) readily available in case of emergency. One idea is to write these numbers on a sticker and put it on all phone receivers.
- Have at least one phone located where it is always accessible. Keep a cordless phone in your pocket at all times. This is especially important if you fall and can't get up to use the phone.
- Make sure smoke detectors work properly.
- Avoid the use of space heaters and electric blankets; these are fire hazards.
How Can Assistive Devices and Adaptive Equipment Help?
Along with appropriate medications, exercise, and other management techniques, adaptive equipment can help you maintain your independence. An occupational therapist or rehabilitation specialist can recommend a variety of assistive devices that are designed to make home care and daily activities more comfortable. Some examples include:
- Built-up utensils
- Grab bars
- Reacher devices
- Electric beds or mattresses
- Sliding boards
- Wheelchairs
How Can I Adapt My Home to Make It Easier to Live In?
Following is a list of the most common recommendations that can help people with Parkinson's disease adapt their home to meet daily challenges.
Note: Not all of these recommendations may benefit your personal situation. Your occupational therapist or rehabilitation specialist can help determine which of these recommendations are best for you.
Tips for Adapting your living room and bedrooms:
- To give yourself plenty of space to move around in, place furniture with wide spaces in between.
- If possible, arrange furniture so outlets are available for lamps and appliances without the need for extension cords. If extension cords are used, make sure they are secured with tape and out of the way so you don't trip on them.
- Use chairs with straight backs, armrests, and firm seats, this will make it much easier for you to get up and sit down. Add firm cushions to existing pieces to add height and make it easier to move.
- Invest in touchable lamps or those that react to sound.
- Adapt your phone by changing the small buttons to larger push buttons to ease dialing. Have frequently called numbers entered into speed dial.
- Install handrails along walls, hallways and stairwells where there is nothing to hold on to.
- Objects such as a stationary pole or "trapeze" bar can be installed if you have difficulty getting out of bed.
- If you have a lot of difficulty getting in and out of bed, try sleeping in a reclining chair.
Tips for adapting your bathroom:
- Use an elevated toilet seat and/or safety rails to assist standing from a low surface. Do not use towel racks or bathroom tissue holders to help you stand.
- Put extended lever handles on faucets to make them easier to turn.
- Install grab bars inside and outside the bathtub or shower.
- Use a bathtub transfer bench or a shower chair with a back support.
- Put a non-skid mat or decals in the bath tub.
- Get rid of small bathroom mats that may cause you to trip, instead purchase a large rug that covers most of the floor, and apply non-stick backing or install wall-to-wall carpeting.
Tips for adapting your kitchen:
- Have at least one counter workspace that has been lowered so you can reach it from a sitting position.
- Use an electric jar opener for tightly sealed containers.
- Don't close jar lids or containers too tight once they have been opened.
- Use an extended lever to assist with lift-tab cans.
- Use pans with a wide base that cannot be knocked over easily.
- Use a food processor for vegetable cutting and peeling.
- Use plastic containers to avoid breakage.
- Use a non-skid mat to stabilize bowls and plates.
- Store food and beverages (such as milk or juice) in small, easy to manage containers.
- Place utensils, pots, pans and measuring cups on a peg board or in an accessible cupboard instead of in lower cupboards which require bending. Sit when getting things out of lower cupboards.
- Use a spike board to stabilize vegetables, fruit, and potatoes so you have both hands free to peel or chop them.
- Use two hands to pour liquids.
- Use scissors to open cellophane packages.
- Use a box top opener to open boxes.
- Use electrical appliances whenever possible.
Other tips:
Make your environment as comfortable and sensory pleasing as possible. Use colors you find soothing to decorate, use scented candles or potpourri in fragrances that relax you.
Keep photos and music around that uplift your spirit. If you find you would like company during the day consider a pet such as a bird, a fish or a cat. If you are concerned about daily care, surround yourself with plants or flowers. Make sure the temperature and climate are suitable to your sensitivities. The more comfortable and uplifting your environment is, the more positive your attitude will be!
Resources
National Parkinson Foundation - http://www.parkinson.org/
Parkinson’s Disease Foundation - http://www.pdf.org/
National Institute of Neurological Disorders and Stroke - http://www.ninds.nih.gov/disorders/parkinsons_disease/parkinsons_disease.htm
A resource for identifying clinical trials funded by the US - http://www.ClinicalTrials.gov
Apathy Evaluation Scale - http://tbims.org/combi/aes/
Works Cited
Aarsland, D., Andersen, K., Larsen, J., & Lolk, A. (2003). Prevalence and Characteristics of Dementia in Parkinson Disease: An 8-Year Prospective Study. Arch Neurol , 60, 387-92.
Braak, H., Del Tredici, K., Bratzke, H., Hamm-Clement, J., Sandmann-Kei, l. D., & Rüb, U. (2002). Staging of the intracerebral inclusion body pathology associated with idiopathic Parkinson's disease (preclinical and clinical stages). J Neurol , 249 Suppl 3, 1-5.
Emre, M., Aarsland, D., & Brown, R. et al. (2007). Clinical diagnostic criteria for dementia associated with. Mov Disord , 22, 1689-1707.
Geotz, C., Tilley, B., Shaftman, S., Stebbins, G., et al. (2008). Movement Disorder Society-sponsored revision of the Unified Parkinson's Disease Rating Scale (MDS-UPDRS): scale presentation and clinimetric testing results. Mov Disord , 2129-70.
Gillingham, F., & Donaldson, M. (1969). Third Symposium of Parkinson's Disease. (pp. 152-7). Edinburgh, Scotland: E&S Livingstone.
Hely, M., Morris, J., Traficante, R., Reid, W., O'Sullivan, D., & Williamson, P. (1999). The sydney multicentre study of Parkinson's disease: progression and mortality at 10 years. J Neurol Neurosurg Psychiatry , 300-7.
Hoehn M, Yahr, M. (1967). Parkinsonism: onset, progression and mortality. Neurology , 427-42.
Kitada, T., Asakawa, S., Hattori, N., Matsumine, H., Yamamura, Y., Minoshima, S., et al. (1998). Mutations in the parkin gene cause autosonal recessive juvenile parkinsonism. Nature , 392, 605-8.
Lau, L., & Breteler, M. (2006). Epidemiology of Parkinson's disease. Lancet Neurol , 5(6), 525-35.
Marin, R., Biedrzycki, R., & Firinciogullar, i. S. (1991). Reliability and validity of the Apathy Evaluation Scale. Psychiatry Res , 38, 143-62.
Marttila, R., & Rinne, U. (1977). Disability and progression in Parkinson's disease. Acta Neurol Scand , 159-69.
Morris, M., Watts, J., Iansek, R., Jolley, D., Campbell, D., Murphy, et al. (2009). Quantifying the profile and progression of impairments, activity, participation, and quality of life in people with Parkinson disease: protocol for a prospective cohort study. BMC Geriatr , 9:2.
Parkinson, J. (1817). An Essay on the Shaking Palsy. London: Whittingham and Rowland.
Perl, D. P. (1998). The Neuropathology of Parkisonian Disorders, Third Edition. In E. T. Joseph Jankovic, Parkinson's Disease and Movement Disorders (pp. 401-18). Baltimore: William and Wilkins.
Pfeiffer, R. (2003). Gastrointestinal dysfunction in Parkinson's disease. Lancet Neurol , 107-16.
Schenk, C., Bundlie, S., & Mahowald, M. (1996). Delayed emergence of parkinsonisn disorder in 38 % of 29 older men initially diagnosed with idiopathic rapid eye movement sleep behavior disorder. Neurology, 46(2), 388-93.
Slaughter, J., Slaughter, K., Nichols, D., Holmes, S., & Martens, M. (2001). Prevalence, Clinical Manifestations, Etiology, and Treatment of Depression in Parkinson's Disease. J Neuropsychiatry Clin Neurosci , 13, 187-96.
Tanner, C., Ottman, R., Goldman, S., et al. (1999). Parkinson disease in twins: an etiologic study. JAMA, 281(4), 341-6.
Appendix - Unified Parkinson's Disease Rating Scale (UPDRS)
I. Mentation, Behavior, Mood
Intellectual Impairment
0-none
1-mild (consistent forgetfulness with partial recollection of events with no other difficulties)
2-moderate memory loss with disorientation and moderate difficulty handling complex problems
3-severe memory loss with disorientation to time and often place, severe impairment with problems
4-severe memory loss with orientation only to person, unable to make judgments or solve problems
Thought Disorder
0-none
1-vivid dreaming
2-"benign" hallucination with insight retained
3-occasional to frequent hallucination or delusions without insight, may interfere with daily activities
4-persistent hallucination, delusions, or florid psychosis.
Depression
0-not present
1-periods of sadness or guilt greater than normal, not sustained for more than a few days or a week
2-sustained depression for >1 week
3-vegetative symptoms (insomnia, anorexia, abulia, weight loss)
4-vegetative symptoms with suicidality
Motivation/Initiative
0-normal
1-less of assertive, more passive
2-loss of initiative or disinterest in elective activities
3-loss of initiative or disinterest in day to say (routine) activities
4-withdrawn, complete loss of motivation
II. Activities of Daily Living
Speech
0-normal
1-mildly affected, no difficulty being understood
2-moderately affected, may be asked to repeat
3-severely affected, frequently asked to repeat
4-unintelligible most of time
Salivation
0-normal
1-slight but noticeable increase, may have nighttime drooling
2-moderately excessive saliva, hay minimal drooling
3-marked drooling
Swallowing
0-normal
1-rare choking
2-occasional choking
3-requires soft food
4-requires NG tube or G-tube
Handwriting
0-normal
1-slightly small or slow
2-all words small but legible
3-severely affected, not all words legible
4-majority illegible
Cutting Food/Handing Utensils
0-normal
1-somewhat slow and clumsy but no help needed
2-can cut most foods, some help needed
3-food must be cut, but can feed self
4-needs to be fed
Dressing
0-normal
1-somewhat slow, no help needed
2-occasional help with buttons or arms in sleeves
3-considerable help required but can do something alone
4-helpless
Hygiene
0-normal
1-somewhat slow but no help needed
2-needs help with shower or bath or very slow in hygienic care
3-requires assistance for washing, brushing teeth, going to bathroom
4-helpless
Turning in Bed/ Adjusting Bed Clothes
0-normal
1-somewhat slow no help needed
2-can turn alone or adjust sheets but with great difficulty
3-san initiate but not turn or adjust alone
4-helpless
Falling-Unrelated to Freezing
0-none
1-rare falls
2-occasional, less than one per day
3-average of once per day
4->1 per day
Freezing When Walking
0-normal
1-rare, may have start hesitation
2-occasional falls from freezing
3-frequent freezing, occasional falls
4-frequent falls from freezing
Walking
0-normal
1-mild difficulty, day drag legs or decrease arm swing
2-moderate difficultly requires no assist
3-severe disturbance requires assistance
4-cannot walk at all even with assist
Tremor
0-absent
1-slight and infrequent, not bothersome to patient
2-moderate, bothersome to patient
3-severe, interfere with many activities
4-marked, interferes with many activities
Sensory Complaints Related to Parkinsonism
0-none
1-occasionally has numbness, tingling, and mild aching
2-frequent, but not distressing
3-frequent painful sensation
4-excruciating pain
III. Motor Exam
Speech
0-normal
1-slight loss of expression, diction,volume
2-monotone, slurred but understandable, mod. impaired
3-marked impairment, difficult to understand
4-unintelligible
Facial Expression
0-Normal
1-slight hypomymia, could be poker face
2-slight but definite abnormal diminution in expression
3-mod. hypomimia, lips parted some of time
4-masked or fixed face, lips parted 1/4 of inch or more with complete loss of expression
*Tremor at Rest
Face
0-absent
1-slight and infrequent
2-mild and present most of time
3-moderate and present most of time
4-marked and present most of time
Right Upper Extremity (RUE)
0-absent
1-slight and infrequent
2-mild and present most of time
3-moderate and present most of time
4-marked and present most of time
LUE
0-absent
1-slight and infrequent
2-mild and present most of time
3-moderate and present most of time
4-marked and present most of time
RLE
0-absent
1-slight and infrequent
2-mild and present most of time
3-moderate and present most of time
4-marked and present most of time
LLE
0-absent
1-slight and infrequent
2-mild and present most of time
3-moderate and present most of time
4-marked and present most of time
Action or Postural Tremor
RUE
0-absent
1-slight, present with action
2-moderate, present with action
3-moderate present with action and posture holding
4-marked, interferes with feeding
LUE
0-absent
1-slight, present with action
2-moderate, present with action
3-moderate present with action and posture holding
4-marked, interferes with feeding
Rigidity
Neck
0-absent
1-slight or only with activation
2-mild/moderate
3-marked, full range of motion
4-severe
RUE
0-absent
1-slight or only with activation
2-mild/moderate
3-marked, full range of motion
4-severe
LUE
0-absent
1-slight or only with activation
2-mild/moderate
3-marked, full range of motion
4-severe
RLE
0-absent
1-slight or only with activation
2-mild/moderate
3-marked, full range of motion
4-severe
LLE
0-absent
1-slight or only with activation
2-mild/moderate
3-marked, full range of motion
4-severe
Finger taps
Right
0-normal
1-mild slowing, and/or reduction in amp.
2-moderate impaired. Definite and early fatiguing, may have occasional arrests
3-severely impaired. Frequent hesitations and arrests.
4-can barely perform
Left
0-normal
1-mild slowing, and/or reduction in amp.
2-moderate impaired. Definite and early fatiguing, may have occasional arrests
3-severely impaired. Frequent hesitations and arrests.
4-can barely perform
Hand Movements (open and close hands in rapid succession)
Right
0-normal
1-mild slowing, and/or reduction in amp.
2-moderate impaired. Definite and early fatiguing, may have occasional arrests
3-severely impaired. Frequent hesitations and arrests.
4-can barely perform
Left
0-normal
1-mild slowing, and/or reduction in amp.
2-moderate impaired. Definite and early fatiguing, may have occasional arrests
3-severely impaired. Frequent hesitations and arrests.
4-can barely perform
Rapid Alternating Movements (pronate and supinate hands)
Right
0-normal
1-mild slowing, and/or reduction in amp.
2-moderate impaired. Definite and early fatiguing, may have occasional arrests
3-severely impaired. Frequent hesitations and arrests.
4-can barely perform
Left
0-normal
1-mild slowing, and/or reduction in amp.
2-moderate impaired. Definite and early fatiguing, may have occasional arrests
3-severely impaired. Frequent hesitations and arrests.
4-can barely perform
Leg Agility (tap heel on ground, amp should be 3 inches)
Right
0-normal
1-mild slowing, and/or reduction in amp.
2-moderate impaired. Definite and early fatiguing, may have occasional arrests
3-severely impaired. Frequent hesitations and arrests.
4-can barely perform
Left
0-normal
1-mild slowing, and/or reduction in amp.
2-moderate impaired. Definite and early fatiguing, may have occasional arrests
3-severely impaired. Frequent hesitations and arrests.
4-can barely perform
Arising From Chair (pt. arises with arms folded across chest)
0-normal
1-slow, may need more than one attempt
2-pushes self up from arms or seat
3-tends to fall back, may need multiple tries but can arise without assistance
4-unable to arise without help
Posture
0-normal erect
1-slightly stooped, could be normal for older person
2-definitely abnormal, mod. stooped, may lean to one side
3-severely stooped with kyphosis
4-marked flexion with extreme abnormality of posture
Gait
0-normal
1-walks slowly, may shuffle with short steps, no festination or propulsion
2-walks with difficulty, little or no assistance, some festination, short steps or propulsion
3-severe disturbance, frequent assistance
4-cannot walk
Postural Stability (retropulsion test)
0-normal
1-recovers unaided
2-would fall if not caught
3-falls spontaneously
4-unable to stand
Body Bradykinesia/ Hypokinesia
0-none
1-minimal slowness, could be normal, deliberate character
2-mild slowness and poverty of movement, definitely abnormal, or dec. amp. of movement
3-moderate slowness, poverty, or small amplitude
4-marked slowness, poverty, or amplitude
IV. Dyskinesias
Duration: What proportion of the waking day are dyskinesias present?
0-none
1-1–25% of day
2-26–50% of day
3-51–75% of day
4-76–100% of day
Disability: How disabling are the dyskinesias?
0- Not disabling
1- Mildly disabling
2- Moderately disabling
3- Severely disabling
4- Completely disabling
Painful Dyskinesias: How painful are the dyskinesias?
0- No painful dyskinesias
1- Slight
2- Moderate
3- Severe
4- Marked
Presence of Early Morning Dystonia: (Historical information)
0- No
1- Yes
Clinical fluctuations
Are any “off” periods predictable as to timing after a dose of medication?
0- No
1- Yes
Are any “off” periods unpredictable as to timing after a dose of medication?
0- No
1- Yes
Do any of the “off” periods come on suddenly, for example, over a few seconds?
0- No
1- Yes
What proportion of the waking day is patient “off” on average?
0-none
1-1–25% of day
2-26–50% of day
3-51–75% of day
4-76–100% of day
Other complications
Does the patient have anorexia, nausea, or vomiting?
0- No
1- Yes
Does the patient have any sleep disturbances, for example, insomnia or hypersomnolence?
0- No
1- Yes
Does the patient have symptomatic orthostasis?
0- No
1- Yes